REGION RESIDENTS USE SOCIAL MEDIA TO FIND ORGANS
|
|
KIDNEY STORIES: DIALYSIS AND DIABETES |



Region residents turn to social media for organs
Giles Bruce
LANSING — Nora Sintich is running out of options.
She's been on the liver transplant waiting list for 14 years, her condition worsening. She can no longer eat bananas, peanuts or pineapples. She uses a walker to get around.
"I don't know how to read anymore. I used to be a bookkeeper — I can't add anymore," said Sintich, a slight, frail woman of 49 who labors when she speaks. "I have trouble with speech. I can't pronounce words right. I never knew the liver was so important."
Then she met a woman who encouraged her to tell her story on social media. Sintich is the opposite of tech savvy — her son equipped her with a personal Facebook page just this past December — but she decided to give it a shot anyway.
Since setting up her page in January, the Lansing grandmother already has received several queries from people interested in donating (donors give a portion of their liver, which regenerates in a matter of months). While the majority were from foreigners offering to sell their livers, a practice illegal in the United States, one came from a woman in Michigan with the same blood type.
As social media proliferates, people on transplant waiting lists are increasingly turning to sites like Facebook and Twitter to find living donors. Social media allows users to broadcast their stories to strangers across the world, at a time when 120,000 Americans await lifesaving transplants.
Dr. Deepak Mital, director of the kidney transplant program at Advocate Christ Medical Center in Oak Lawn, said more and more people on the list at his facility have been taking to social media.
He noted that all living donors have to go through a rigorous evaluation process, meeting with a social worker and psychologist, to ensure they're doing it for the right reasons.
"We apply the same standards to donors who come through social media as those who came through personal contact," he said. "You have to make sure there was no coercion, no financial exchange and that this is all on the up and up."
+10
Gary resident Jim Myers receives dialysis while looking at social media pages dedicated to connecting organ donors with recipients. John J. Watkins, The Times
When Jim Myers, of Gary, started dialysis about five years ago, he was dismayed by all the suffering he saw around him, by the number of people unable to speak for themselves. Active in social media since the days of MySpace, Myers decided to start a Facebook page called Kidney Stories to spread awareness about kidney disease. He now administers about 30 pages for people in need of organ transplants.
"I've done all the other stuff: knocked on doors, manned tables. At an event, I might reach 25 to 50 people," said the former college professor. "On social media, I'm reaching close to 100,000 people a week."
Subtitles
On a recent day at a Dyer dialysis clinic, Myers typed at his laptop with his right hand, his left arm hooked up to blood-filled tubes leading to a machine that filtered the toxins out of his body.
"This is one I opened this week," Myers said, pointing to his computer screen, his browser open to dozens of pages. "The guy's from Georgia. I've got him up to 119 likes in a couple days."
Last year, Myers won the inaugural Social Media and Advocacy Award from the American Association of Kidney Patients. "I'm on three transplant lists. I have good doctors that look after me," he said. "I hope to find my own donor, but I really enjoy helping other people."
Inspired by her dad receiving a liver transplant five years ago, Laurie Lee, of Cary, Ill., now tries to help others make similar connections. After meeting Sintich recently, she helped set up her Facebook page, Looking for a Liver for Nora.
"Right now, with millennials, they're altruistic and looking to help people," said Lee, 35. "And those are the people on social media. There's a ton of potential."
A family photograph of Nora Sintich, left, her brother John Medina and her sister Teresa Rivera, who died from liver disease when she was 40. In the photograph from 2008 Nora's head is shaved after she had brain surgery. Liver disease is hereditary in Nora's family. Jonathan Miano, The Times \
Sintich is willing to give it a try. Several of her loved ones have been tested to see if they'd be candidates, to no avail. Her condition has progressed, but not to the point where she'd move to the top of the waiting list.
She has a hereditary form of cirrhosis of the liver, a disease that took the life of her sister at the age of 40. She also has hepatic encephalopathy, a decline in brain function, as well as a movement disorder.
"I've spent so much time in the hospital, the nurses call me the frequent flyer," she said.
But her doctors have told her her health would largely return to normal with a successful transplant. If that happens, she plans to volunteer for a Chicago-based transplant organization and her husband, Doug, intends to donate his liver to a stranger.
"My grandma made it to 98. I tell my dad I'm going to beat grandma," she said. "I fight because I have two granddaughters (5 and 2). I tell my son I'll be at their college graduation."
http://www.nwitimes.com/niche/get-healthy/health-care/region-residents-turn-to-social-media-for-organs/article_5b44f05c-66f6-56aa-a9f0-c2f8efbd3411.html
Giles Bruce
- Updated 8 hrs ago
LANSING — Nora Sintich is running out of options.
She's been on the liver transplant waiting list for 14 years, her condition worsening. She can no longer eat bananas, peanuts or pineapples. She uses a walker to get around.
"I don't know how to read anymore. I used to be a bookkeeper — I can't add anymore," said Sintich, a slight, frail woman of 49 who labors when she speaks. "I have trouble with speech. I can't pronounce words right. I never knew the liver was so important."
Then she met a woman who encouraged her to tell her story on social media. Sintich is the opposite of tech savvy — her son equipped her with a personal Facebook page just this past December — but she decided to give it a shot anyway.
Since setting up her page in January, the Lansing grandmother already has received several queries from people interested in donating (donors give a portion of their liver, which regenerates in a matter of months). While the majority were from foreigners offering to sell their livers, a practice illegal in the United States, one came from a woman in Michigan with the same blood type.
As social media proliferates, people on transplant waiting lists are increasingly turning to sites like Facebook and Twitter to find living donors. Social media allows users to broadcast their stories to strangers across the world, at a time when 120,000 Americans await lifesaving transplants.
Dr. Deepak Mital, director of the kidney transplant program at Advocate Christ Medical Center in Oak Lawn, said more and more people on the list at his facility have been taking to social media.
He noted that all living donors have to go through a rigorous evaluation process, meeting with a social worker and psychologist, to ensure they're doing it for the right reasons.
"We apply the same standards to donors who come through social media as those who came through personal contact," he said. "You have to make sure there was no coercion, no financial exchange and that this is all on the up and up."
+10
Gary resident Jim Myers receives dialysis while looking at social media pages dedicated to connecting organ donors with recipients. John J. Watkins, The Times
When Jim Myers, of Gary, started dialysis about five years ago, he was dismayed by all the suffering he saw around him, by the number of people unable to speak for themselves. Active in social media since the days of MySpace, Myers decided to start a Facebook page called Kidney Stories to spread awareness about kidney disease. He now administers about 30 pages for people in need of organ transplants.
"I've done all the other stuff: knocked on doors, manned tables. At an event, I might reach 25 to 50 people," said the former college professor. "On social media, I'm reaching close to 100,000 people a week."
Subtitles
- subtitles off
- captions off
- Chapters
On a recent day at a Dyer dialysis clinic, Myers typed at his laptop with his right hand, his left arm hooked up to blood-filled tubes leading to a machine that filtered the toxins out of his body.
"This is one I opened this week," Myers said, pointing to his computer screen, his browser open to dozens of pages. "The guy's from Georgia. I've got him up to 119 likes in a couple days."
Last year, Myers won the inaugural Social Media and Advocacy Award from the American Association of Kidney Patients. "I'm on three transplant lists. I have good doctors that look after me," he said. "I hope to find my own donor, but I really enjoy helping other people."
Inspired by her dad receiving a liver transplant five years ago, Laurie Lee, of Cary, Ill., now tries to help others make similar connections. After meeting Sintich recently, she helped set up her Facebook page, Looking for a Liver for Nora.
"Right now, with millennials, they're altruistic and looking to help people," said Lee, 35. "And those are the people on social media. There's a ton of potential."
A family photograph of Nora Sintich, left, her brother John Medina and her sister Teresa Rivera, who died from liver disease when she was 40. In the photograph from 2008 Nora's head is shaved after she had brain surgery. Liver disease is hereditary in Nora's family. Jonathan Miano, The Times \
Sintich is willing to give it a try. Several of her loved ones have been tested to see if they'd be candidates, to no avail. Her condition has progressed, but not to the point where she'd move to the top of the waiting list.
She has a hereditary form of cirrhosis of the liver, a disease that took the life of her sister at the age of 40. She also has hepatic encephalopathy, a decline in brain function, as well as a movement disorder.
"I've spent so much time in the hospital, the nurses call me the frequent flyer," she said.
But her doctors have told her her health would largely return to normal with a successful transplant. If that happens, she plans to volunteer for a Chicago-based transplant organization and her husband, Doug, intends to donate his liver to a stranger.
"My grandma made it to 98. I tell my dad I'm going to beat grandma," she said. "I fight because I have two granddaughters (5 and 2). I tell my son I'll be at their college graduation."
http://www.nwitimes.com/niche/get-healthy/health-care/region-residents-turn-to-social-media-for-organs/article_5b44f05c-66f6-56aa-a9f0-c2f8efbd3411.html
KIDNEY STORIES: WHO GETS THE KIDNEY?

Who Gets the Kidney? 5 Changes to the
Allocation System
Posted
on July 11,
2013 by nkf _advocacy
More than 96,000 Americans are currently on the waiting list for a
life-saving kidney and if this year follows the trend of years past, there will
only be about 16,500 kidneys donated. Clearly, the demand is far greater than
the supply and therefore, no policy for allocating donor kidneys can possibly
match every patient in need with a donor. However, when it comes to deceased
donor transplants, recently announced changes to the allocation rules are an
improvement over the current system. These changes were made by the Organ
Procurement and Transplant Network (OPTN) and the United Network for Organ
Sharing (UNOS).
1) Priority for the Most
Highly-Sensitized
Transplant candidates who are only likely to match with 0-2% of deceased
donors (CPRA score of 100%-98%) because they are
highly-sensitized will be placed at the top of the kidney transplant wait list
in order to help increase their chance of receiving a transplant.
Candidates with a less than 1% likelihood of matching (CPRA score of 100%)
will also get first priority at receiving a kidney from anywhere in the country
if that kidney couldn’t be matched to a highly-sensitized patient with a CPRA
score of 100-98% in the local transplant unit or region where the organ was
donated. While these candidates are still likely to remain on the list for
five or more years, this new prioritization will provide them more opportunities
to receive a transplant than under the current system.
In addition, under the new policy, candidates with a CPRA score of 20% or
above will be assigned priority points that will help improve their chance at
receiving a transplant when a match is available.
2) Blood Type B and Minority
Access
People on the waiting list whose blood type is B will be able to receive
kidneys from donors with blood types A2 and
A2B under the new policy. However, not
all candidates with type B blood can successfully accept a kidney from
A2 and A2B
donors, so the candidate will first have to undergo a blood test to see how
their body will respond to a donation with these blood types.
Since many minorities have blood type B, expanding the blood types from which
type B candidates can receive donor kidneys may slightly increase the number of
minorities receiving kidney transplants. This can, help reduce racial
disparities in access to kidney transplantation.
3) Improvements to the Waitlist
The new policy sets back the clock for adults 18 years and older who are on
the transplant waiting list to the day they started dialysis. Candidates
will still be able to accrue time on the wait list when registered with a GFR of
20 ml/minute or less. So regardless of when a patient is actually
evaluated for the transplant waiting list, once they are placed on the list,
their time spent on dialysis counts in regards to how they are prioritized on
the list. This policy reduces disparities in transplantation among the
under-served who may not have been prepared to pursue the option of
transplantation when first starting dialysis. For children under 18,
waitlist time is established based on the day they registered for a kidney
transplant or the day they began dialysis, whichever occurred first.
Children will still be able to accrue waiting time without being on
dialysis.
4) Life-Expectancy Matching for the Top 20%
of Kidneys
The new policy will match recipients and deceased donors
according to the “life expectancy” of the kidney in about 20% of the kidneys.
Candidates who are expected to need a kidney for the longest amount of time will
be matched with the kidneys expected to function the longest.
This policy scores deceased donor kidneys using the kidney donor profile
index (KDPI) to determine how long the kidney is expected to last.
Transplant candidates are also scored using the Estimated Post-transplant
Survival (EPTS). The EPTS is not a score based solely on age, but on other
health factors such as whether the patient had received a prior transplant,
diabetes status and time on dialysis.
While it is likely that mostly younger, healthier patients will end up with
lower EPTS scores and receive priority for the kidneys with a KDPI between 0-20%
(the top 20% of kidneys expected to function the longest), this policy will
encourage more efficient matching of donated kidneys. It may also reduce
the number of repeat transplants for these recipients. In addition,
candidates will have to consent to receive a kidney in the bottom 15% (a KDPI of
85% or higher) since these kidneys are expected to have a shorter functioning
life span than kidneys with a lower KDPI. Kidneys with a KDPI of 85% or higher
will also be offered to a wider geographic area. For those candidates who are
more likely to immediately benefit from a transplant rather than remain on
dialysis, this will allow quicker access to a kidney transplant.
5) Priority for Living Organ
Donors
In the rare instances where a living donor (of any organ or part of an organ)
needs a kidney transplant, they will also be given priority assignment for
organs with any KDPI score, including those in the top 20%. The National
Kidney Foundation believes prioritizing prior living organ donors is ethical and
fairly honors the gift they made.
Exceptions
While rarely used, a transplant physician’s right to
give a donated kidney out of order, due to medical urgency is protected under
this policy. However, all physicians in the local transplant region must agree
to the change.
The National Kidney Foundation anticipates that this new kidney allocation
policy will protect the gift of life. The policy will extend the length of
time a transplanted kidney functions for a recipient, improve equity in the
waitlist and improve the ability for those with rare blood types and high
sensitivity to receive a deceased donor transplant.
However, there are still too few kidney donors to meet the needs of the more
than 96,000 patients on the kidney transplant waitlist. Learn more about organ donation today!
Allocation System
Posted
on July 11,
2013 by nkf _advocacy
More than 96,000 Americans are currently on the waiting list for a
life-saving kidney and if this year follows the trend of years past, there will
only be about 16,500 kidneys donated. Clearly, the demand is far greater than
the supply and therefore, no policy for allocating donor kidneys can possibly
match every patient in need with a donor. However, when it comes to deceased
donor transplants, recently announced changes to the allocation rules are an
improvement over the current system. These changes were made by the Organ
Procurement and Transplant Network (OPTN) and the United Network for Organ
Sharing (UNOS).
1) Priority for the Most
Highly-Sensitized
Transplant candidates who are only likely to match with 0-2% of deceased
donors (CPRA score of 100%-98%) because they are
highly-sensitized will be placed at the top of the kidney transplant wait list
in order to help increase their chance of receiving a transplant.
Candidates with a less than 1% likelihood of matching (CPRA score of 100%)
will also get first priority at receiving a kidney from anywhere in the country
if that kidney couldn’t be matched to a highly-sensitized patient with a CPRA
score of 100-98% in the local transplant unit or region where the organ was
donated. While these candidates are still likely to remain on the list for
five or more years, this new prioritization will provide them more opportunities
to receive a transplant than under the current system.
In addition, under the new policy, candidates with a CPRA score of 20% or
above will be assigned priority points that will help improve their chance at
receiving a transplant when a match is available.
2) Blood Type B and Minority
Access
People on the waiting list whose blood type is B will be able to receive
kidneys from donors with blood types A2 and
A2B under the new policy. However, not
all candidates with type B blood can successfully accept a kidney from
A2 and A2B
donors, so the candidate will first have to undergo a blood test to see how
their body will respond to a donation with these blood types.
Since many minorities have blood type B, expanding the blood types from which
type B candidates can receive donor kidneys may slightly increase the number of
minorities receiving kidney transplants. This can, help reduce racial
disparities in access to kidney transplantation.
3) Improvements to the Waitlist
The new policy sets back the clock for adults 18 years and older who are on
the transplant waiting list to the day they started dialysis. Candidates
will still be able to accrue time on the wait list when registered with a GFR of
20 ml/minute or less. So regardless of when a patient is actually
evaluated for the transplant waiting list, once they are placed on the list,
their time spent on dialysis counts in regards to how they are prioritized on
the list. This policy reduces disparities in transplantation among the
under-served who may not have been prepared to pursue the option of
transplantation when first starting dialysis. For children under 18,
waitlist time is established based on the day they registered for a kidney
transplant or the day they began dialysis, whichever occurred first.
Children will still be able to accrue waiting time without being on
dialysis.
4) Life-Expectancy Matching for the Top 20%
of Kidneys
The new policy will match recipients and deceased donors
according to the “life expectancy” of the kidney in about 20% of the kidneys.
Candidates who are expected to need a kidney for the longest amount of time will
be matched with the kidneys expected to function the longest.
This policy scores deceased donor kidneys using the kidney donor profile
index (KDPI) to determine how long the kidney is expected to last.
Transplant candidates are also scored using the Estimated Post-transplant
Survival (EPTS). The EPTS is not a score based solely on age, but on other
health factors such as whether the patient had received a prior transplant,
diabetes status and time on dialysis.
While it is likely that mostly younger, healthier patients will end up with
lower EPTS scores and receive priority for the kidneys with a KDPI between 0-20%
(the top 20% of kidneys expected to function the longest), this policy will
encourage more efficient matching of donated kidneys. It may also reduce
the number of repeat transplants for these recipients. In addition,
candidates will have to consent to receive a kidney in the bottom 15% (a KDPI of
85% or higher) since these kidneys are expected to have a shorter functioning
life span than kidneys with a lower KDPI. Kidneys with a KDPI of 85% or higher
will also be offered to a wider geographic area. For those candidates who are
more likely to immediately benefit from a transplant rather than remain on
dialysis, this will allow quicker access to a kidney transplant.
5) Priority for Living Organ
Donors
In the rare instances where a living donor (of any organ or part of an organ)
needs a kidney transplant, they will also be given priority assignment for
organs with any KDPI score, including those in the top 20%. The National
Kidney Foundation believes prioritizing prior living organ donors is ethical and
fairly honors the gift they made.
Exceptions
While rarely used, a transplant physician’s right to
give a donated kidney out of order, due to medical urgency is protected under
this policy. However, all physicians in the local transplant region must agree
to the change.
The National Kidney Foundation anticipates that this new kidney allocation
policy will protect the gift of life. The policy will extend the length of
time a transplanted kidney functions for a recipient, improve equity in the
waitlist and improve the ability for those with rare blood types and high
sensitivity to receive a deceased donor transplant.
However, there are still too few kidney donors to meet the needs of the more
than 96,000 patients on the kidney transplant waitlist. Learn more about organ donation today!
TAGS: CMS, Cuts to dialysis centers
funding, kidney, kidney donations, kidney failure, kidney transplant, kidneystories, National Kidney
Foundation, polycystic kidney
disease, UNOS and tagged awareness, blood, chronic kidney disease, diabetic, dialysis, donate life, donor, End Stage Renal Failure, Facebook, find a kidney for, fundraiser, Indiana University, Jim Myers, kidney, kidney disease, kidney for, Kidney Stories, Live Journal, living kidney donor, National Kidney Foundation, NCS,
Ning, organ donation, polycystic kidney disease, recipient, save my life, seeking, share a spare, sharing, transfusion, transplant list, Tumblr, UNOS, Weebly, WordPress by kidneystories
funding, kidney, kidney donations, kidney failure, kidney transplant, kidneystories, National Kidney
Foundation, polycystic kidney
disease, UNOS and tagged awareness, blood, chronic kidney disease, diabetic, dialysis, donate life, donor, End Stage Renal Failure, Facebook, find a kidney for, fundraiser, Indiana University, Jim Myers, kidney, kidney disease, kidney for, Kidney Stories, Live Journal, living kidney donor, National Kidney Foundation, NCS,
Ning, organ donation, polycystic kidney disease, recipient, save my life, seeking, share a spare, sharing, transfusion, transplant list, Tumblr, UNOS, Weebly, WordPress by kidneystories
KIDNEY STORIES: THE NATIONAL KIDNEY FOUNDATION'S 10 YEAR PLAN TO END THE WAIT
http://www.youtube.com/watch?v=3TrW5bRlX9s&feature=player_embedded#action=share
The National Kidney Foundation’s 10 year plan to End the Wait:
Organ
Donation & Transplantation RECOMMENDATIONS
Improve Outcomes of First
Transplants
Financial - Cover immunosuppressive drugs for life
Education - Educate CKD Stage 4 patients about
staying as healthy as they
can
the opportunities for and benefits of early transplantation
the
possibility of living donations and
… the identification of potential living
donors
Medical Practice -
Evaluate Stage 4 CKD patients for a
transplant prior to the initiation of dialysis
Increase Deceased
Donation
Financial - Ensure that OPOs have the discretion and funding to
assist donor families with expenses directly related to the donation, which may
include some funeral expenses
Education - Facilitate awareness of all
appropriate hospital personnel about the optimal care for potential donor
families
Medical Practice -
Minimize discard and maximize
utilization of donated organs
Identify, recover and utilize organs from
Extended Criteria Donors and from Donation after Cardiac Death donors nationwide
Increase Living Donation
Financial -
Guarantee that all living
donors, without qualification, are reimbursed for all expenses involved in the
donation, including lost wages. This includes non-directed donors and potential
donors who are evaluated but don’t ultimately donate.
Guarantee living
donors access to health care coverage for any medical expense or disability
related to the donation
Guarantee living donors life insurance coverage for
death related to the donation
Guarantee that living donors get their jobs,
or equivalent jobs, back
Guarantee that living donors will not be
discriminated against in obtaining health and life insurance
Establish a
specific billing code for post-donation care of living donors
Education -
Create an NKF Living Donor Council to support the needs of living donors
and potential donors
Create a “Living Donation Breakthrough Collaborative"
to stimulate best practices for living donation
Inform the general public
about new developments in living donation and transplantation
Medical
Practice -
Increase staff and physical resources at transplant centers to
minimize the time waiting for a living donation
Evaluate more than one
potential living donor for a single recipient when feasible
Collect,
maintain and analyze data on living donors annually, consisting of, at least,
blood pressure, eGFR, proteinuria and Hb A1C
Make the donation and
transplant system and processes more efficient and equitable Medical Practice -
Eliminate regional variations in the rates of consent, living donations,
early transplantation, access to transplantation and follow-up care
Eliminate racial and other disparities in donating, listing, remaining active on
the waiting list and receiving a transplant
Maintain uniform organ donation
laws across the United States
THE NKF CONTENDS THAT IF THEY ARE SUCCESSFUL WITH THIS INITIATIVE, A PERSON
ON THE LIST WILL NOT HAVE TO WAIT MORE THAN 1 YEAR ON THE LIST!
http://www.youtube.com/watch?v=3TrW5bRlX9s&feature=player_embedded#action=share
The National Kidney Foundation’s 10 year plan to End the Wait:
Organ
Donation & Transplantation RECOMMENDATIONS
Improve Outcomes of First
Transplants
Financial - Cover immunosuppressive drugs for life
Education - Educate CKD Stage 4 patients about
staying as healthy as they
can
the opportunities for and benefits of early transplantation
the
possibility of living donations and
… the identification of potential living
donors
Medical Practice -
Evaluate Stage 4 CKD patients for a
transplant prior to the initiation of dialysis
Increase Deceased
Donation
Financial - Ensure that OPOs have the discretion and funding to
assist donor families with expenses directly related to the donation, which may
include some funeral expenses
Education - Facilitate awareness of all
appropriate hospital personnel about the optimal care for potential donor
families
Medical Practice -
Minimize discard and maximize
utilization of donated organs
Identify, recover and utilize organs from
Extended Criteria Donors and from Donation after Cardiac Death donors nationwide
Increase Living Donation
Financial -
Guarantee that all living
donors, without qualification, are reimbursed for all expenses involved in the
donation, including lost wages. This includes non-directed donors and potential
donors who are evaluated but don’t ultimately donate.
Guarantee living
donors access to health care coverage for any medical expense or disability
related to the donation
Guarantee living donors life insurance coverage for
death related to the donation
Guarantee that living donors get their jobs,
or equivalent jobs, back
Guarantee that living donors will not be
discriminated against in obtaining health and life insurance
Establish a
specific billing code for post-donation care of living donors
Education -
Create an NKF Living Donor Council to support the needs of living donors
and potential donors
Create a “Living Donation Breakthrough Collaborative"
to stimulate best practices for living donation
Inform the general public
about new developments in living donation and transplantation
Medical
Practice -
Increase staff and physical resources at transplant centers to
minimize the time waiting for a living donation
Evaluate more than one
potential living donor for a single recipient when feasible
Collect,
maintain and analyze data on living donors annually, consisting of, at least,
blood pressure, eGFR, proteinuria and Hb A1C
Make the donation and
transplant system and processes more efficient and equitable Medical Practice -
Eliminate regional variations in the rates of consent, living donations,
early transplantation, access to transplantation and follow-up care
Eliminate racial and other disparities in donating, listing, remaining active on
the waiting list and receiving a transplant
Maintain uniform organ donation
laws across the United States
THE NKF CONTENDS THAT IF THEY ARE SUCCESSFUL WITH THIS INITIATIVE, A PERSON
ON THE LIST WILL NOT HAVE TO WAIT MORE THAN 1 YEAR ON THE LIST!
TAGS: Ning, Live Journal, Tumblr, Weebly, WordPress, Facebook, Kidney Stories, Jim
Myers, kidney, dialysis, blood, transfusion, donor, recipient, seeking,
awareness, National Kidney Foundation, Indiana University, sharing, kidney
disease, End Stage Renal Failure, polycystic kidney disease, chronic kidney
disease, kidney for, diabetic, save my life, living kidney donor, organ
donation, find a kidney for, NCS, share a spare, transplant list, fundraiser,
donate life, END THE WAIT
Myers, kidney, dialysis, blood, transfusion, donor, recipient, seeking,
awareness, National Kidney Foundation, Indiana University, sharing, kidney
disease, End Stage Renal Failure, polycystic kidney disease, chronic kidney
disease, kidney for, diabetic, save my life, living kidney donor, organ
donation, find a kidney for, NCS, share a spare, transplant list, fundraiser,
donate life, END THE WAIT
NEWS
Here we post news about organ and kidney donation, organizations, medical and scientific articles, coaches, speakers, vacations, advocacy, events and inspirational photos. Browse our news page and get caught up!
THIS IS AN INTERVIEW WITH ANGELA VUJKO CONCERNING BLAKE LOUDENBER (MIRCALE FOR BLAKE ON FACEBOOK) https://www.facebook.com/AMiracleForBlake/info
BLAKE'S KIDNEY STORY:
Meet Blake Loudenber. He is a nine year old from Griffith, Indiana who has
been waiting almost eight years for his second kidney transplant. Blake was
born with Polycystic Kidney Disease (PKD). Infants born with this disease have
a low survival rate. Thankfully, Blake has defeated most odds and will be
turning 10 in April. When Blake was born doctors had no hope of him surviving.
One of his doctors wanted to send him home to die. However, Blake’s other
doctor felt that he could save his life by putting him on dialysis. At 3 weeks
old, Blake was the youngest patient to be put on dialysis through the
University of Chicago. They saved his life.
At the age of
two Blake received his first kidney transplant. He was doing well for a short
while. Unfortunately, Blake soon became very ill. He was so sick that he could
not even lift his head up. His family would walk him around for hours and hours
just to keep him happy. He never cried, he never moaned, he would not talk, not
a sound. What made this worse was Blake could not even walk yet; he was just
lying there, dying. His family was in despair, they were scared they were going
to lose him. All they could do was watch his little soul dwindle away. Through
all this though, they still had hope.
One day, Blake took
an even further turn for the worse. He was sitting up at the counter eating and
he fell over almost hitting the floor. There was no response from him. When the
ambulance arrived, they just ran in, and immediately ran out with Blake. They
rushed him to Community Hospital in Munster, Indiana. The doctors told Blake’s
family that there was nothing more that could be done. Blake was dying. His
little body was filled up with toxins and those toxins had put his body into
shock. Finally, doctors decided to air lift him to Chicago and told his family
that they should say their goodbyes because he probably would not make it
there. They watched him take off and that was it. They thought Blake was gone.
They drove to the hospital in Chicago in complete silence.
The helicopter arrived in Chicago and they immediately
rushed Blake in to the hospital. Even though they thought he would not make it,
they decided to insert a breathing tube into Blake. At this point Blake was
unable to breathe on his own. Cindy, Blake’s grandmother and caregiver, stayed
the night with him at the hospital. Around five o’clock in the morning
something amazing happened. Blake was beginning to breathe a little bit on his
own. Things were beginning to look up for this young boy. It took a long time
but Blake finally pulled through. The doctors said it was a true miracle.
Blake was put back on dialysis and back on the kidney transplant list. Due to his age, Blake is at the top of the list. He has waited almost 8 long years now and still has not received his second kidney transplant. Blake has waited longer than any child in need of a kidney that has been treated out of the University of Chicago. There are two reasons why. The first reason is his blood type. Blake’s blood type is O positive. Anyone with that blood type can only accept forms of O blood. The second reason is because his body rejected the first kidney transplant. His antibodies shot sky high and it makes it extremely difficult for his blood to accept anything. Blake’s aunt Kylee was a match for him, but when they mixed the blood there was a bad reaction and that ruled her out.
During the wait of
finding a match, he has suffered from many infections throughout the years.
Most of these infections are from his dialysis catheter and they can be very
hard to clear up. During Christmas 2011, he had a really bad infection and
barely pulled through it. He was in the hospital for almost a month. He had
many painful surgeries during this time. Blake has also had numerous blood
transfusions and takes many medications orally and through injections. Due to a
severe reaction to growth hormones, Blake’s growth plates are nearly closed. He
has not grown since the age of four and a half. If Blake does not get a
transplant before these plates close, he will remain 3 ½ feet for the rest of
his life.
Every night we send our children to bed, have
them brush their teeth, and take care of their regular night time rituals.
Blake, on the other hand, has to be hooked up to his dialysis machine. He has
to be on the machine for 11 hours every evening. Waking up the next day, he
knows he cannot just jump out of bed and start his day. He has to finish his
dialysis, take his medications, and then get ready for school. When you see
Blake playing, he is running around and laughing like a normal kid. He loves
baseball and plays little league and basketball. He goes to school, complains
about homework, and does what an all American kid does. The only holdback is
his illness. His aunt Kelly asked him what he would like to tell the world. His
response was, “everything is going to be ok.” Blake is only 9 right now. His
aunt Kelly does not think Blake realizes what it means when they say he may
never grow. “Right now, he’s just a shorty, but still loves life. My biggest
fear is that he’ll never grow, and that will lead to a shorter life, and that
one day he won’t keep smiling about everything. We need his smile”(Kelly Ray).
Blake has a large family who he lives with. They revolve
their lives around Blake. He has had a few miracles in his life but the
grandest one of all is the love that his family has for each other. His grandma
Cindy says that Blake’s favorite thing is rainbows. He really loves drawing
them. He draws her one every day. This is a sign to her that he believes
somewhere, somehow, there is a bright side to all of this. Her fear is that if
the rainbows start disappearing, his hope will diminish. It is very important
to her that he keeps drawing those rainbows. Blake’s doctor told her to
remember that when he is out playing that he is not a normal kid. He will
always need special care and love. He is a miracle.
Blake
needs a kidney immediately. He is a truly amazing child and deserves a fair
shot at a normal healthy life. He is a child that has endured so much pain,
more than most adults have dealt with in their lifetime. Please help this
little man get his kidney so the rainbows do not disappear.
If you are interested in seeing if you are a match for
Blake please visit the University of Chicago’s website:
http://www.uchospitals.edu/specialties/transplant/kidney/donate.html
Please fill out the health questionnaire and the application
and send it back to The University of Chicago
For more
information about Blake, please visit our Facebook page:
https://www.facebook.com/AMiracleForBlake
Originally
written By: Joan Vujko Rohrman
Revised By: Angela Vujko
been waiting almost eight years for his second kidney transplant. Blake was
born with Polycystic Kidney Disease (PKD). Infants born with this disease have
a low survival rate. Thankfully, Blake has defeated most odds and will be
turning 10 in April. When Blake was born doctors had no hope of him surviving.
One of his doctors wanted to send him home to die. However, Blake’s other
doctor felt that he could save his life by putting him on dialysis. At 3 weeks
old, Blake was the youngest patient to be put on dialysis through the
University of Chicago. They saved his life.
At the age of
two Blake received his first kidney transplant. He was doing well for a short
while. Unfortunately, Blake soon became very ill. He was so sick that he could
not even lift his head up. His family would walk him around for hours and hours
just to keep him happy. He never cried, he never moaned, he would not talk, not
a sound. What made this worse was Blake could not even walk yet; he was just
lying there, dying. His family was in despair, they were scared they were going
to lose him. All they could do was watch his little soul dwindle away. Through
all this though, they still had hope.
One day, Blake took
an even further turn for the worse. He was sitting up at the counter eating and
he fell over almost hitting the floor. There was no response from him. When the
ambulance arrived, they just ran in, and immediately ran out with Blake. They
rushed him to Community Hospital in Munster, Indiana. The doctors told Blake’s
family that there was nothing more that could be done. Blake was dying. His
little body was filled up with toxins and those toxins had put his body into
shock. Finally, doctors decided to air lift him to Chicago and told his family
that they should say their goodbyes because he probably would not make it
there. They watched him take off and that was it. They thought Blake was gone.
They drove to the hospital in Chicago in complete silence.
The helicopter arrived in Chicago and they immediately
rushed Blake in to the hospital. Even though they thought he would not make it,
they decided to insert a breathing tube into Blake. At this point Blake was
unable to breathe on his own. Cindy, Blake’s grandmother and caregiver, stayed
the night with him at the hospital. Around five o’clock in the morning
something amazing happened. Blake was beginning to breathe a little bit on his
own. Things were beginning to look up for this young boy. It took a long time
but Blake finally pulled through. The doctors said it was a true miracle.
Blake was put back on dialysis and back on the kidney transplant list. Due to his age, Blake is at the top of the list. He has waited almost 8 long years now and still has not received his second kidney transplant. Blake has waited longer than any child in need of a kidney that has been treated out of the University of Chicago. There are two reasons why. The first reason is his blood type. Blake’s blood type is O positive. Anyone with that blood type can only accept forms of O blood. The second reason is because his body rejected the first kidney transplant. His antibodies shot sky high and it makes it extremely difficult for his blood to accept anything. Blake’s aunt Kylee was a match for him, but when they mixed the blood there was a bad reaction and that ruled her out.
During the wait of
finding a match, he has suffered from many infections throughout the years.
Most of these infections are from his dialysis catheter and they can be very
hard to clear up. During Christmas 2011, he had a really bad infection and
barely pulled through it. He was in the hospital for almost a month. He had
many painful surgeries during this time. Blake has also had numerous blood
transfusions and takes many medications orally and through injections. Due to a
severe reaction to growth hormones, Blake’s growth plates are nearly closed. He
has not grown since the age of four and a half. If Blake does not get a
transplant before these plates close, he will remain 3 ½ feet for the rest of
his life.
Every night we send our children to bed, have
them brush their teeth, and take care of their regular night time rituals.
Blake, on the other hand, has to be hooked up to his dialysis machine. He has
to be on the machine for 11 hours every evening. Waking up the next day, he
knows he cannot just jump out of bed and start his day. He has to finish his
dialysis, take his medications, and then get ready for school. When you see
Blake playing, he is running around and laughing like a normal kid. He loves
baseball and plays little league and basketball. He goes to school, complains
about homework, and does what an all American kid does. The only holdback is
his illness. His aunt Kelly asked him what he would like to tell the world. His
response was, “everything is going to be ok.” Blake is only 9 right now. His
aunt Kelly does not think Blake realizes what it means when they say he may
never grow. “Right now, he’s just a shorty, but still loves life. My biggest
fear is that he’ll never grow, and that will lead to a shorter life, and that
one day he won’t keep smiling about everything. We need his smile”(Kelly Ray).
Blake has a large family who he lives with. They revolve
their lives around Blake. He has had a few miracles in his life but the
grandest one of all is the love that his family has for each other. His grandma
Cindy says that Blake’s favorite thing is rainbows. He really loves drawing
them. He draws her one every day. This is a sign to her that he believes
somewhere, somehow, there is a bright side to all of this. Her fear is that if
the rainbows start disappearing, his hope will diminish. It is very important
to her that he keeps drawing those rainbows. Blake’s doctor told her to
remember that when he is out playing that he is not a normal kid. He will
always need special care and love. He is a miracle.
Blake
needs a kidney immediately. He is a truly amazing child and deserves a fair
shot at a normal healthy life. He is a child that has endured so much pain,
more than most adults have dealt with in their lifetime. Please help this
little man get his kidney so the rainbows do not disappear.
If you are interested in seeing if you are a match for
Blake please visit the University of Chicago’s website:
http://www.uchospitals.edu/specialties/transplant/kidney/donate.html
Please fill out the health questionnaire and the application
and send it back to The University of Chicago
For more
information about Blake, please visit our Facebook page:
https://www.facebook.com/AMiracleForBlake
Originally
written By: Joan Vujko Rohrman
Revised By: Angela Vujko

KIDNEY STORIES: NEW MEDS FOR TRANSPLANT RECIPIENTS?
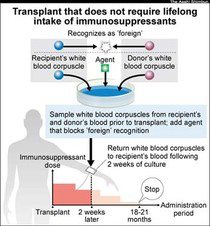
HOW IT WORKS...
HOW NURSES ARE PAID AFFECTS YOUR CARE!
By Alvin Tran
March 1st, 2013, 1:06 PM
Many nurse practitioners say restrictive payment policies impact how they
care for patients more than state laws governing what care they can give,� according
to a new study.
In the study, published Thursday by the National Institute for Health Care Reform,
researchers found that while so-called “scope of practice” laws did not appear to
restrict the primary care services nurse practitioners can provide to patients,
they do affect how the advanced nurses are paid.
Researchers at the Center for Studying Health System
Change conducted telephone interviews with 30 nurse practitioners, practice
managers, and physicians working in a variety of clinical settings — all of
which employed nurse practitioners. The researchers focused on six states
representing a range of legal scope-of-practice restrictions: Maryland,
Arizona, Michigan, Indiana, Massachusetts, and Arkansas.
Based on the interviews, Dr. Tracy Yee and her colleagues found that
nurse practitioners — registered nurses with advanced degrees — faced greater
challenges in the states with more restrictions on how they practice. In states
such as Arkansas and Indiana where they cannot practice without a doctor’s
supervision, nurse practitioners are not recognized as primary care providers by
the traditional Medicaid program, and that affects how they deliver care to
patients as well as how they are paid.
Other challenges in more restrictive states
include disentangling the billing system involving public and private payers,
ordering tests and procedures, and establishing independent primary care
practices. And though private and public payers must adhere to scope-of-practice
laws, they often impose additional restrictions on how these nurse practitioners
practice, the study found.
Many nurse practitioners told researchers that restrictive payment policies
had a much greater impact on their day-to-day practice than the current
scope-of-practice laws enacted in their states. “Payers are in a position to
determine what services NPs are paid for, their payment rates, whether NPs are
designated as primary care providers and assigned their own patient panels, and
whether NPs can be paid directly,” the authors of the study wrote.
Such policies “might hamper the efficiency of our provider capacity,” Yee
said. “NPs can be doing more; they could be seeing more patients; they could be
reaching communities that are underserved more often.”
States might consider making clearer what nurse practitioners can and can’t
bill for — particularly in Medicaid and from other private payers, Yee
added.
Dr. Angela Golden, president of the American Association of Nurse
Practitioners, says she wasn’t surprised by the study’s findings on
scope-of-practice laws. “It’s really important for people to recognize that
removing those outdated laws will especially help people in medically
underserved areas,” she said. “Fifty-five million people live in medically
underserved areas.”
But Dr. Reid Blackwelder, the president-elect of the American Academy of
Family Physicians, said he believes a more collaborative approach among
physicians, advanced practice nurses, and physician assistants would pay
dividends. “This discussion is often tied to the concept that an [advanced
practice nurse] does what a family physician does or takes the place of a family
physician. … What’s really important is that these roles are not interchangeable
— they’re different,” he said during an interview. “Each is critical and
each has a role to play. You can’t just take one and make due if you can’t have
the other.”
This entry was posted on Friday, March 1st,
2013 at 1:06 pm.
www.facebook.com/kidneystories
